In our effort to continue online Undergraduate & postgraduate teaching during COVID 19 lockdown we were pleased to have the live webinar directly from the U.K on:-
4th May 2020 MONDAY from 8.30 pm to 9.30 pm (Indian standard time) By Dr Tasaduk Khan Pulmonologist NHS
TOPIC:
The Lessons learnt while managing COVID-19 patients in the UK Hospital
In our effort to continue online postgraduate teaching during COVID 19 lockdown we are pleased to have the live webinar on 27th April 2020 from 4.30 pm to 5.30pm
TOPIC: Approach to Peripheral Neuropathy
by Prof Prabha Adhikari
Speaker :
Dr Prabha Adhikari, M.D. General Medicine,
PGDGM, Fellow of Indian college of physicians &
Fellow of Geriatric Society of India.
Professor of General Medicine and HOD Geriatric Medicine
Yenepoya Deemed to be University
Former Professor and Dr TMA Pai Endowment Chair in Geriatrics, Manipal University
In our effort to continue online postgraduate teaching during COVID 19 lockdown we are pleased to have the live webinar on 24th April 2020 from 5pm to 6pm
TOPIC: Approach to acute febrile illness in Tropical region : Focus on acute undifferentiated illnesses
Faculty: Prof. Anurag Bhargava, M.D.(Medicine), M.Sc.(Epidemiology)
Professor, Department of Medicine, Yenepoya Medical College
University Road, Deralakatte
Mangalore-575018, Karnataka
Adjunct Professor, Department of Medicine,
McGill University, Montreal, Canada
Prof. Anurag Bhargava,
Trained in Internal Medicine at AIIMS, New Delhi and did a Masters in Epidemiology from McGill University
Currently Professor of Medicine, Yenepoya Medical College, Head, Center for Nutrition Studies,
Yenepoya University and Adjunct Professor, Department of Medicine, McGill University, Montreal.
Member, Strategic Advisory Group of Experts on In-vitro Diagnostics, WHO (SAGE-IVD) for the year 2019-20.
Member, Technical Working Group on TB and Co-morbidities, Central TB Division, Government of India.
Recipient of the British Medical Journal (India) Research Paper of the Year award in 2014.
30 years of clinical experience at all levels of care in India. Spent 10 years as a public health physician in central India, serving rural and tribal communities.
Published more than 35 research papers in journals including
British Medical Journal, American Journal of Respiratory and Critical Care Medicine, International
Journal of Tuberculosis and Lung Disease, Journal of Clinical Tuberculosis and other mycobacterial diseases, PLoS One.
This webinar is based on the following article published in the BMJ:
Bhargava A, Ralph R, Chatterjee B, Bottieau E. Assessment and initial management of acute undifferentiated fever in tropical and subtropical regions. British Medical Journal 2018;363:k4766
A 31-year male an accountant by profession, presented with a persistent cough of six weeks duration. The cough was dry and he denied any history of allergy in the past or any chronic medication. The patient is a non-smoker and also denied any loss of appetite or loss of weight or close contact with any sick patient. There was no history of fever, sweating. He had no change in his voice. There was no history of palpitations, PND or orthopnea. No history of Tuberculosis in the past. Examination: He had stable vitals and normal oxygen saturation on room air.Chest examination: Trachea in the center , The percussion note was normal and on auscultation, there were no added sounds, normal bronchovesicular breath sounds were heard all over.CVS: S1 and S2 were normally heard There was no murmur, rub or gallop Abdomen: Normal CNS: Normal Evaluation and Hospital course: The Hemoglobin levels were 14gm/dl and WBC count and platelets were normal. ESR was 4 mm in the first hour. The tests on Kidney and liver function were normal. Chest X-ray PA view was unremarkable Keeping in view his nagging cough CT scan chest was done as shown in Fig 1 : A cystic lesion at the azygocaval junction was noted. No other lesions were seen
Fig. 1 Cystic hygroma in CT chest
The patient was subjected to Video-assisted thoracoscopic surgery (VATS) and the lesion was resected. It turned out to be Cystic hygroma. The patient had a marked relief and is following our clinic Teaching message :
A normal X-ray chest doesn’t rule out all pathological processes in the symptomatic patient. Further reading click the link: Cystic Hygroma
A 35-year-old male farmer had noticed a swelling of the left side of his hypochondrium that persisted for six months. He had no history of severe abdominal pain, jaundice or fever. There was no history of loss of appetite or weight loss.
Examination:
The patient was conscious and oriented. Icterus, lymphadenopathy, and edema were absent. The examination of his abdomen revealed a swelling that measured 5×6 cm. The swelling was smooth and cystic. In order to confirm the origin of this swelling different maneuvers were used. The swelling disappeared while raising his head suggesting an intraabdominal nature of the swelling. The patient was asked to assume the knee-elbow position and the swelling was palpated in this position. The said swelling disappeared confirming the retroperitoneal nature of this swelling. There was no bruit on auscultation. The results of the systemic examination were normal.
Evaluation:
He had normal levels of hemoglobin(Hb= 13.6gm/dl), white cell count and erythrocyte sedimentation rate were normal as well.
Tests of kidney and liver function were normal and serum amylase levels were not increased. His
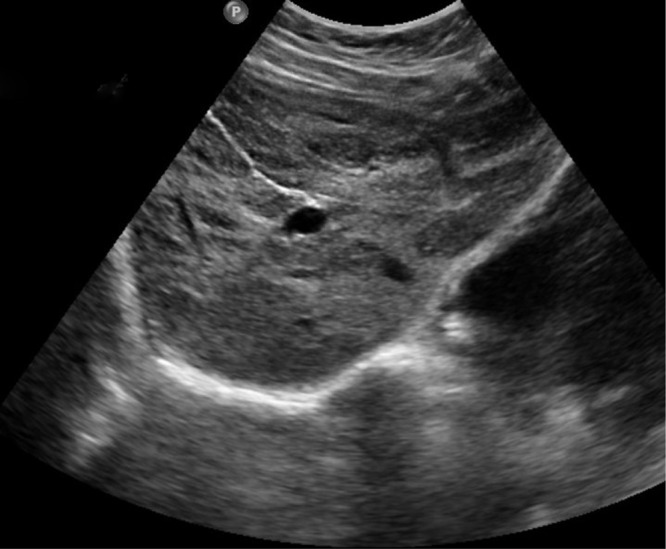
chest X-ray was normal. On ultrasound examination, there was a 7×6 cm swelling surrounding the
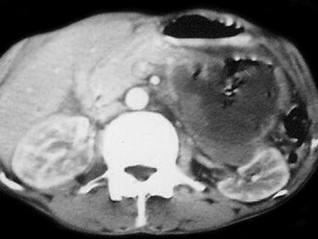
pancreas was documented. The liver, gallbladder and other organs were normal. His abdominal computed tomography
Fig1 CT scan showing Hydatid pancreas
(CT) revealed a cyst in the tail of the pancreas but the pancreatic duct was not dilated. The cyst was 5×6 cm in diameter, and had jagged margins but did not contain daughter cysts. All other organs were normal (Figure 1). No additional cystic lesions were seen in any other organ. IgG antibodies to E. granulosus were detected by enzyme-linked immunosorbent assay (ELISA).
Course: The patient was given albendazole 15 mg/kg perioperatively, and distal pancreatectomy and enucleation of the cyst with proper precautions were done to prevent anaphylaxis. Splenectomy was also performed and hemostasis was achieved. A drain was left in place after the procedure. Histopathology was suggestive of a hydatid cyst.The patient had high blood sugars postoperatively and was managed with insulin subcutaneously. He had an uneventful course. He was discharged from the hospital after eight days. The patient’s blood sugars are under control with insulin. The patient was monitored for six months in our outpatient department.
Teaching message :
The hydatid cyst may be considered as one of the differential diagnosis in the cystic lesions of the pancreas
A 27-year-old male with no significant comorbidities presented with a history of episodic, recurrent abdominal pain of 4 years duration.The patient described the pain as colicky, remaining for 1–2 hours necessitating intravenous analgesics predominantly in the upper abdomen. His abdominal pain had no reference or radiation and there was no jaundice associated with it. The patient had been admitted four times in various hospitals during this period and every time basic laboratory evaluation including liver function tests and serum amylase were within normal limits. His ultrasound examination had been within normal limits on each occasion he was hospitalized for his abdominal pain. The patient denied any high-risk behavior or drug abuse. Over this period he had a stable appetite and constant weight. On examination, he was conscious oriented and he had stable vitals. There was no icterus or lymphadenopathy. His systemic examination was unremarkable.
Evaluation and course :
Laboratory data revealed normal hemogram, normal liver function tests, and his abdominal ultrasound was also within normal limits. There were no eggs or ova in his stool examination. Keeping in view recurrent biliary colics magnetic resonance cholangiopancreatography (MRCP) was done which showed a doubtful filling defect in the common bile duct but intra-hepatic biliary radicals were not dilated. There were no gall stones and the rest of the viscera were within normal limits.
Endoscopic retrograde cholangiopancreatography (ERCP) was undertaken which revealed normal papilla. Selective common bile duct (CBD) cannulation was done and cholangiogram revealed a filling defect in the lower end of the common bile duct. There was mild dilatation of the common bile duct (Figure 1 (Fig. 1)) however, biliary radicals were not dilated.
Fig1 ERCP shows CBD dilatation
Sphincterotomy was done and CBD was swept with a biliary balloon and a live Fasciola hepatica was seen coming out of the common bile duct (Figure 2 (Fig. 2), Figure 3 (Fig. 3)).
Fig 2 Fasciola removed Fig 3 Live Fasciola removed
Later using biopsy forceps the worm was taken out of duodenum and confirmation of the species, Fasciola hepatica was made by the microbiology department of the hospital. Patient was given two tablets of triclabendazole 250 mg (manufactured by Novartis) after the procedure. Following therapeutic ERCP patient became symptom-free and is attending our clinic for last 24 months now.
Teaching message :
Fascioliasis is one of the unusual causes of recurrent biliary colics and it warrants a high degree of clinical suspicion especially in non-endemic areas. The current report emphasizes that ERCP may be considered for management of recurrent biliary colics even though classical features of biliary obstruction may not be present.
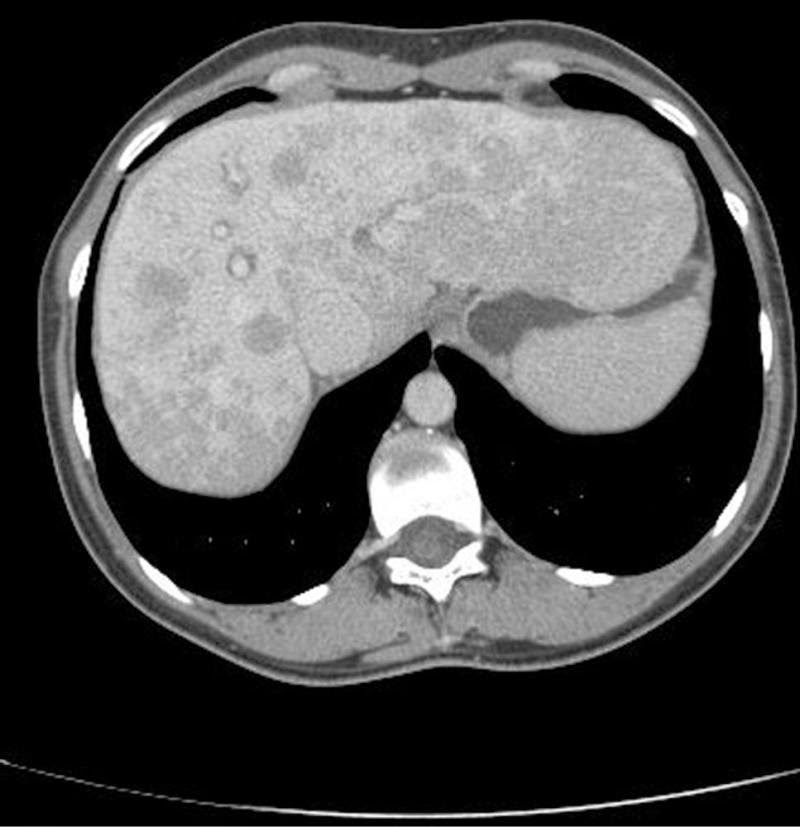
Clinical scenario: A 39-year-old female presented with a CT scan report, that read, ” multiple hypodense lesions in the liver suggestive of metastasis liver. The gall bladder, Hepatic veins, portal vein are normal. No lesion in the CBD and intrahepatic ducts are also normal”. The patient was admitted for evaluation of the primary after explaining poor prognosis to her husband thoroughly. On examination, she was conscious, oriented and deeply Jaundiced. Her vitals were stable. Her systemic examination was unremarkable.
Laboratory tests showed normal hemogram but ESR (erythrocyte sedimentation rate )was raised at 52 mm/H (normal, 0-20 mm/H). She had an elevated INR 2.7 Her liver function tests revealed predominantly conjugated hyperbilirubinemia [Bilirubin 12 mg/dl )] elevated liver enzymes (AST aspartate aminotransferase: 818U/L and ALT 51 5 U/L). Serum alkaline phosphatase levels were also elevated at 327 IU/L /L All her viral markers were negative.
Fig 1 CT scan showing Metastasis Liver
All tumor markers CA -125, CEA and Alpha fetoproteins were elevated. For the search of the primary an upper GI endoscopy, colonoscopy including a mamogram was carried out. All turned out to be normal. While the search for the primary was on , day 4th of admission the patient was found to be incoherent, talking irrelevantly. Her arterial ammonia levels were high and she was shifted to ICU and managed as hepatic encephalopathy. Gladly , her sensorium improved after 3 days and a liver biopsy was planned for evaluation of liver lesions. Keeping in view her high INR 4 units of FFP were transfused and transjugular liver biopsy was done.The Liver biopsy was suggestive of Autoimmune hepatitis a great surprise to one and all.
She was given oral steroids and her Liver function tests improved. Repeat Ultrasound of the abdomen showed clearance of liver lesions
Fig.2 USG abdomen showing no liver lesion post treatment
One year later she was the mother of her 3rd baby.
Take-Home message
Focal liver lesions are more often discovered with the widespread use of diagnostic imaging modalities. Despite tremendous advancements in the field of radiology, radiological features are not definite. Treat the patient and not an investigation report.
A 57-year-old male patient, waiter by occupation without any previous comorbidities,
came with complaints of the frontal headache of one-week duration
It was associated with, low-grade fever & chills.
The patient also complained of swaying to the left side while walking
which affected his job in the hotel.
There were no similar complaints in the past, no history of prior trauma, head injury, fall or recent vaccination.No history of seizures.No history of loss of weight or appetite.
On examination: The patient’s vitals and general physical examination were normal.
CNS examination revealed normal higher mental function.
The cranial nerves, motor system, sensory, examination were normal.
The fundus examination was also normal.
He had no signs of meningeal irritation.
However, there was the presence of bilateral cerebellar signs in the form of ataxia,
dysdiadochokinesia, fingernoseataxia more on the left side than the right.
The patient had classical cerebellar gait,
Other system examination was normal.
Evaluation
On evaluation, the patient had normal Complete blood count
Hb- 14g%, TLC-8000cells/mm3, platelets, ESR eosinophils we’re in a normal range.
RBS, LFT, RFT were normal. The serology for HIV, HBsAg was negative.
MRI brain revealed multifocal ring-enhancing lesions in supra and infratentorial neuroparenchyma with diffuse cerebral edema suggestive of neurocysticercosis.
(Fig 1)
CSF fluid analysis showed protein 17 mg%, glucose 91mg%, cell count of 18 with neutrophil predominance. CSF ADA was within normal limits.
The ZN stain of CSF was negative for AFB.
Hospital course:
His GCS at presentation was 15. The patient was Treated with anti-edema measures Mannitol, dexamethasone 8 mg thrice a day.
However during the course of hospital stay patient had a drop in GCS to E4M5V4,
CT brain was done showed obstructive hydrocephalus and a ventriculoperitoneal shunt
was placed to decompress the brain.
On Post-op day 3 patient’s sensorium improved and
he was discharged home a few days later
Teaching message
Bilateral cerebellar signs are more common with systemic diseases
like post-infectious cerebellitis, multiple sclerosis, ADEM.
But in tropical areas, parasitic infestation should also be considered
as a differential for acute ataxia.
Fig2 Neurocystiscircosis in cerebellar region .
\Acute ataxia is an uncommon presentation of neurocysticercosis.
The Yenepoya Pre University College, Jeppinamogeru, had a tremendous season this year clinching all the major soccer titles in the district. They won the Independence Cup organised by the District Football Association. They lifted the District level Trophy and six members of the team represented the State level Football Tournament. They finished Runners Up in the State and six members of the Yenepoya PU College got selected for the Nationals.
It gives us immense pleasure to inform you that our football team won the ‘Independence Cup’ organised by D.K football association. 28 teams from the different colleges of D.K District competed for the trophy. The strength, hard work and dedication of our students brought us this success.
We congratulate all the team players for their excellent performance. Special thanks to Mr. Bibi Thomas (coach) and Mr. Sujith K V (Physical Education Director) and for their efforts and training our students to be able to achieve this prestigious trophy!!
All the best for future games and best wishes from management, teachers and students.