Dear Friends Sharing this article published 21 March 2020
Beating corona as a doctor
Singapore has not had a single health care related transmission of corona virus. No, they did NOT use universal N95 masks or full body protective gear for every patient contact. They did NOT use hydroxychloroquine either. Similar success story has been achieved in Honk Kong. What can we learn from this ?
Social distancing within hospitals and clinics
Waiting room chairs 6 feet apart. Doctor and patient 6 feet apart. Doctors should wear surgical masks. No role for cloth masks.
Who needs N95 masks?
The use of N95 masks, face-protectors, goggles, and gowns are reserved for procedures where respiratory secretions can be aerosolized (for example, intubating a patient for anesthesia) and for known or suspected cases of COVID-19.
If your coworker becomes unexpectedly positive, the worker and his “close” contacts will be quarantined. Who is a “close”contact?
In Hong Kong, “close contact” means fifteen minutes at a distance of less than six feet and without the use of a surgical mask; in Singapore, thirty minutes. If the exposure is shorter than the prescribed limit but within six feet for more than two minutes, workers can stay on the job if they wear a surgical mask and have twice-daily temperature checks. What this means is it is possible to cut down transmission to nearly zero even without unproven prophylaxis even if you are a healthcare worker at high risk. (Source: Adapted from Atul Gawande in NYT on Mar 21)
Dear Friends: The schools and colleges have been closed due to CORONAEPIDAMIC
But we can still teach online so that our younger generation doesn’t suffer during these tough times.
Yesterday attended a workshop on ONLINE CLASS at our University. Thanks to Deputy Director IT Yenepoya Medical College Hospital Mr Rajesh
Sharing my experience: How to set up an online class :
Step 1 Create a Google account and let all your students have their Gmail. Step 2: Click on the calendar and create an event Click ADD CONFERENCING Step 3 Share your class code with students. Step 4 Share your PowerPoint presentation with class up to 250 students Here you go !!! Start teaching from your home and let students be at their respective homes Stay safe and avoid #corona . Prevention is the only way as there is still no cure Thanks to science and technology
Thanks to our respected speakers for making Haemocon 2020 successful
Dr. Govind Eriat M.B.BS, DNB (INTERNAL MEDICINE) FRCP GLASGOW) Fellow Leukemia/ BMT Program of British Columbia (Vancouver) Senior Consultant, Division of Hematology and Bone marrow Transplant, Meitra Hospital, Calicut. Kerala Adjunct faculty, Faculty of Internal Medicine, Yenepoya University, Mangalore.
Dr. Mahadeva swamy B C Consultant Hematologist and BMT physician. Manipal-hospital-Goa.
MBBS, MD (Med), DNB (Clin.Hemat)2017 DNB CLINICAL HEMATOLOGY (NAT BOARD Delhi). 2018 Fellowship in Haematology CMC-Vellore.2014 – MD (General Medicine). Kasturba Medical College & Government Wenlock hospital, Mangalore. Manipal university, Karnataka.
PRESENTATIONS & PUBLICATIONS Research Studies: 1. “Estimation of Peripheral Blood CD34 count of subjects undergoing Stem Cell Harvest after giving Growth Factors and Harvest yield CD34 count” 2. Correlation of Type 2 Diabetes Mellitus duration with the severity of coronary artery disease Gensini score.Poster presentation:At EBMT, Marseille , France ,2017
1. Outcome comparison of hematopoietic stem cell transplant performed in HEPA and non-HEPA filter rooms: experience from a single centre in India 2. Cost effective outcome of generic medicines used in CyBorD protocol induction and generic Melphalan Autologous transplant conditioning: A single centre experience in 25 patients of Multiple Myeloma.At hematocrit 2016. 1. Total Knee Arthroplasty in Patients with Hemophilia: Single Centre experience in western India. 2. “Allogeneic hematopoietic stem cell transplantation for Beta-thalassemia major in the developing world: Experience from a center in western India” Click to download the lecture
Dr. Prashantha B Head of the Dept Adult Hematology at KMC Mangalore DNB Medicine: Narayana Hrudayalaya, Bangalore 2009 Fellowship in Hematology: Mazumdar Shaw Cancer Centre, Narayana Health City, Bangalore
Started the first-ever dedicated Hematology center in Mangalore in 2012 at KMC Hospital. Since then, heading the dept of Adult Hematology at KMC
Areas of interest: Hematological disorders of elderly, acute leukemia, Myelodysplastic syndromes and myeloproliferative disorders. He has multiple articles to his credit. He conducts social oriented health education programs regularly. He has been conducting yearly CME s for the benefit of fellow colleague doctors.He is the member secretary for the Association of Medical Consultants, Mangalore for the year 2019-2020.
Dr. Rajesh Krishna,MD, MRCP, FRCPath (U.K) CCT Hematology (U.K)
Consultant Hematoncologist, YMCH, MangaloreMBBS in Govt medical college Calicut followed by MD Gen Med at Madras medical college and then went to UK in 2004Completed MRCP and joined for 5 year higher training in Haematology in London including Hammersmith hospital and University college London during which time attained FRC Path and CCT haematology with dual training in both clinical and laboratory Haematology apart from bone marrow transplantation.Worked as Consultant in UK for almost 6 years. Special interest in Dysproteinaemias such as myeloma and WM. Performed over 100 myeloma related stem cell transplants and presented over 30 abstracts in conferences.
A 37-year-old female presented with a history of epigastric pain of 8 weeks duration. The pain had an intensity of 7/10 and was a burning type of pain with no reference or radiation. She stated that for the previous 2 weeks her pain was aggravated by food intake. She denied any alarming symptoms in the form of loss of appetite and weight loss. There was no history of vomiting or melena. Her clinical examination was normal
Evaluation: Her hemoglobin levels were 14 g/dl. She had a normal leukocyte count, and liver function and renal function were normal. Serum lipase and amylase levels were not elevated. An ultrasound of her abdomen did not indicate the presence of gallstones and all other organs were normal. She underwent upper gastrointestinal (GI) endoscopy to rule out a gastric ulcer due to the pain being aggravated by food. An upper gastroscopic examination revealed normal esophagus. There was 5 cm × 4 cm bulge in the antral portion of her stomach, and the overlying mucosa was erythematosus [Figure 1]. The fundus and body of the stomach were normal. There was no evidence of duodenal ulcer or growth. A biopsy from the antral portion revealed chronic gastritis, but there was no evidence of Helicobacter pylori.
Fig.1 Endoscopic picture EGD Antrum
She underwent endoscopic ultrasound (EUS) due to the nodular lesion. The EUS showed a round intramural (subepithelial) lesion in the antrum of the stomach. The lesion was hypoechoic and seemed to appear from the submucosa and measured 30 mm in diameter. The outer endoscopic borders were well-defined. The EUS did not show any lymph nodes in the vicinity, and the liver was normal. The differential diagnosis of gastrointestinal tumor (GIST) was considered and fine needle aspiration was performed after color Doppler imaging ruled out the presence of vascular structures along the needle track. However, the microscopic examination showed no evidence of malignancy and immune cytochemistry for K-ras was negative for GIST.
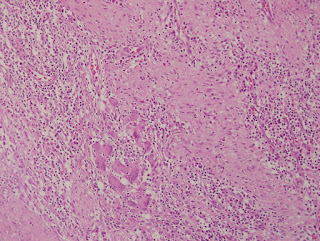
Fig. Histology Pancreatic rest
Abdominal computerized tomography confirmed that apart from a submucosal lesion in the pylorus of the stomach all other organs were normal on imaging. As a result of the mass lesion in the stomach, the patient underwent partial gastrectomy determine the nature of this gastric lesion as fine needle aspiration had not clearly identified the lesion. The microscopic examination of the resected portion identified islands of pancreatic acini and ducts in the muscularis propria of the stomach. Several dilated ducts were seen extending through all the layers of the muscularis propria. There was evidence of fibrotic reaction and scant mixed inflammatory infiltrate was observed in the area. There was no evidence of malignancy and the immunocytochemistry CA19-9 was positive in the tissue while CK20 chromogranin was negative in the specimen. The overall microscopic features were consistent with pancreatic rest and GIST was ruled out.(Fig 2) The patient had an uneventful postoperative course and was discharged home after 6 days of hospitalization. She was prescribed oral proton pump inhibitors 20 mg once daily for 1-month duration only. The patient, who did not take any medication for this complaint after the initial proton pump inhibitors, is now pain-free. She has been followed up by the clinic for the last 2 years.
Further reading :
The pancreatic rest, is an uncommon congenital anomaly .The incidence in autopsy series varies from 1 to 2% (range 0.55 to 13%). Such tissue may occur throughout the gastrointestinal tract but has a propensity to affect the stomach and the proximal small intestine. Histological features of acinar formation, development of ducts and independent blood supply are usually present . Accordingly four types have been described ,type I having more resemblance to normal pancreatic tissue and type IV showing only islets cells . Although cause of pancreatic rest remains unclear, several theories, including the ‘theory of metaplasia,’ the ‘theory of misplacement’ and the latest addition, the ‘theory of abnormalities of notch signaling’, have been proposed to explain the pathogenesis and occurrence of pancreatic heterotopia. While majority of patients with pancreatic ectopic tissue are asymptomatic, a variety of symptoms are attributed to this ectopic tissue . Depending upon location and bulk of the pancreatic rest the symptoms may include , gastrointestinal bleeding, gastric outlet obstruction, gastric ulceration, pancreatitis and even obstructive jaundice, when located near Ampulla of vater have been described .There are reports when such lesions have presented with acute perforation , what may reflect pancreatitis of stomach and duodenum . When discovered during endoscopic examination it is very important to differentiate these lesions from submucosal tumors and appropriate surgery may be required to confirm the lesion when results of fine needle aspiration are inconclusive .Despite the advent of novel diagnostic modalities, including endoscopic ultrasonography (EUS), computer tomography (CT) and even EUS-guided fine-needle aspiration (EUS-FNA), the differentiation from a neoplasm at times remains a clinical challenge . When in a given case FNAC has proved it to be pancreatic rest and the patient is asymptomatic , such lesions can be monitored . Endoscopic features of this rare entity and a brief review is presented in this report .
A 35-year-old male farmer had noticed a swelling of the left side of his hypochondrium that persisted for six months. He had no history of severe abdominal pain, jaundice or fever. There was no history of loss of appetite or weight loss.
Examination:
The patient was conscious and oriented. Icterus, lymphadenopathy, and edema were absent. The examination of his abdomen revealed a swelling that measured 5×6 cm. The swelling was smooth and cystic. In order to confirm the origin of this swelling different maneuvers were used. The swelling disappeared while raising his head suggesting an intraabdominal nature of the swelling. The patient was asked to assume the knee-elbow position and the swelling was palpated in this position. The said swelling disappeared confirming the retroperitoneal nature of this swelling. There was no bruit on auscultation. The results of the systemic examination were normal.
A 31-year male an accountant by profession, presented with a persistent cough of six weeks duration. The cough was dry and he denied any history of allergy in the past or any chronic medication. The patient is a non-smoker and also denied any loss of appetite or loss of weight or close contact with any sick patient. There was no history of fever, sweating. He had no change in his voice. There was no history of palpitations, PND or orthopnea. No history of Tuberculosis in the past. Examination: He had stable vitals and normal oxygen saturation on room air.Chest examination: Trachea in the center , The percussion note was normal and on auscultation, there were no added sounds, normal bronchovesicular breath sounds were heard all over.CVS: S1 and S2 were normally heard There was no murmur, rub or gallop Abdomen: Normal CNS: Normal Evaluation and Hospital course: The Hemoglobin levels were 14gm/dl and WBC count and platelets were normal. ESR was 4 mm in the first hour. The tests on Kidney and liver function were normal. Chest X-ray PA view was unremarkable Keeping in view his nagging cough CT scan chest was done as shown in Fig 1 : A cystic lesion at the azygocaval junction was noted. No other lesions were seen
Fig. 1 Cystic hygroma in CT chest
The patient was subjected to Video-assisted thoracoscopic surgery (VATS) and the lesion was resected. It turned out to be Cystic hygroma. The patient had a marked relief and is following our clinic Teaching message :
A normal X-ray chest doesn’t rule out all pathological processes in the symptomatic patient. Further reading click the link: Cystic Hygroma
A 35-year-old male farmer had noticed a swelling of the left side of his hypochondrium that persisted for six months. He had no history of severe abdominal pain, jaundice or fever. There was no history of loss of appetite or weight loss.
Examination:
The patient was conscious and oriented. Icterus, lymphadenopathy, and edema were absent. The examination of his abdomen revealed a swelling that measured 5×6 cm. The swelling was smooth and cystic. In order to confirm the origin of this swelling different maneuvers were used. The swelling disappeared while raising his head suggesting an intraabdominal nature of the swelling. The patient was asked to assume the knee-elbow position and the swelling was palpated in this position. The said swelling disappeared confirming the retroperitoneal nature of this swelling. There was no bruit on auscultation. The results of the systemic examination were normal.
Evaluation:
He had normal levels of hemoglobin(Hb= 13.6gm/dl), white cell count and erythrocyte sedimentation rate were normal as well.
Tests of kidney and liver function were normal and serum amylase levels were not increased. His
chest X-ray was normal. On ultrasound examination, there was a 7×6 cm swelling surrounding the
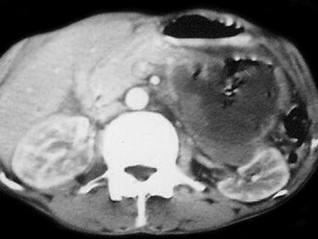
pancreas was documented. The liver, gallbladder and other organs were normal. His abdominal computed tomography
Fig1 CT scan showing Hydatid pancreas
(CT) revealed a cyst in the tail of the pancreas but the pancreatic duct was not dilated. The cyst was 5×6 cm in diameter, and had jagged margins but did not contain daughter cysts. All other organs were normal (Figure 1). No additional cystic lesions were seen in any other organ. IgG antibodies to E. granulosus were detected by enzyme-linked immunosorbent assay (ELISA).
Course: The patient was given albendazole 15 mg/kg perioperatively, and distal pancreatectomy and enucleation of the cyst with proper precautions were done to prevent anaphylaxis. Splenectomy was also performed and hemostasis was achieved. A drain was left in place after the procedure. Histopathology was suggestive of a hydatid cyst.The patient had high blood sugars postoperatively and was managed with insulin subcutaneously. He had an uneventful course. He was discharged from the hospital after eight days. The patient’s blood sugars are under control with insulin. The patient was monitored for six months in our outpatient department.
Teaching message :
The hydatid cyst may be considered as one of the differential diagnosis in the cystic lesions of the pancreas
A 27-year-old male with no significant comorbidities presented with a history of episodic, recurrent abdominal pain of 4 years duration.The patient described the pain as colicky, remaining for 1–2 hours necessitating intravenous analgesics predominantly in the upper abdomen. His abdominal pain had no reference or radiation and there was no jaundice associated with it. The patient had been admitted four times in various hospitals during this period and every time basic laboratory evaluation including liver function tests and serum amylase were within normal limits. His ultrasound examination had been within normal limits on each occasion he was hospitalized for his abdominal pain. The patient denied any high-risk behavior or drug abuse. Over this period he had a stable appetite and constant weight. On examination, he was conscious oriented and he had stable vitals. There was no icterus or lymphadenopathy. His systemic examination was unremarkable.
Evaluation and course :
Laboratory data revealed normal hemogram, normal liver function tests, and his abdominal ultrasound was also within normal limits. There were no eggs or ova in his stool examination. Keeping in view recurrent biliary colics magnetic resonance cholangiopancreatography (MRCP) was done which showed a doubtful filling defect in the common bile duct but intra-hepatic biliary radicals were not dilated. There were no gall stones and the rest of the viscera were within normal limits.
Endoscopic retrograde cholangiopancreatography (ERCP) was undertaken which revealed normal papilla. Selective common bile duct (CBD) cannulation was done and cholangiogram revealed a filling defect in the lower end of the common bile duct. There was mild dilatation of the common bile duct (Figure 1 (Fig. 1)) however, biliary radicals were not dilated.
Fig1 ERCP shows CBD dilatation
Sphincterotomy was done and CBD was swept with a biliary balloon and a live Fasciola hepatica was seen coming out of the common bile duct (Figure 2 (Fig. 2), Figure 3 (Fig. 3)).
Fig 2 Fasciola removed Fig 3 Live Fasciola removed
Later using biopsy forceps the worm was taken out of duodenum and confirmation of the species, Fasciola hepatica was made by the microbiology department of the hospital. Patient was given two tablets of triclabendazole 250 mg (manufactured by Novartis) after the procedure. Following therapeutic ERCP patient became symptom-free and is attending our clinic for last 24 months now.
Teaching message :
Fascioliasis is one of the unusual causes of recurrent biliary colics and it warrants a high degree of clinical suspicion especially in non-endemic areas. The current report emphasizes that ERCP may be considered for management of recurrent biliary colics even though classical features of biliary obstruction may not be present.









{kind=link}
{kind=link}
{kind=link}
{kind=link}