

Clinical scenario :
A 60-year-old male presented with complaints of easy fatigability of 3 months duration .it was followed by a fever of 3 weeks duration Fever was not associated with Rigors and Chills more so in the evenings. The patient also complained of reduced appetite and weight loss-16kgs in 3 months. Before the current presentation, he developed progressive deterioration in his sensorium and vomiting. The vomiting was not bilious, not blood-tinged usually the food taken by him earlier. There was no history of cough with expectoration, no history of diarrhea, no dysphagia No history of diabetes, hypertension in the past or any other comorbidity
On examination:The patient was irritable and disoriented to time, place and person Pallor was present Generalised emaciation,BMI – 18.2kg/m2.No icterus, clubbing, cyanosis, pedal edema, lymphadenopathy Pulse rate- 100 bpm – Regular Rhythm BP- 110/90 mmHg RR- 23 cycles per minute Found to have polyuria during input-output monitoring RS: No accessory muscles used, B/L Reduced breath sounds at base of the lung P/A : Umbilicus appears normal, distended abdomen, No organomegaly, and bowel sounds heard, On Percussion – Shifting Dullness (+) CNS: No focal neurological deficit Differential diagnosis considered were : Chronic Infections-Tuberculosis/HIV Malignancy-hematological/gastrointestinal/lung Endocrine-diabetes, hyperthyroidism, hyperparathyroidism
INVESTIGATIONS CBC-Hb-9.4 g/dL ,TLC 5.5 X 103 /µL,Neutrophil-79.6% (25-50%)Lymphocyte 12.8% (25-40%)Eosinophil 1.8% (1-6%)Basophil0.4% (0-1%)Monocyte5.4% (1-8%) Blood sugars-normal, TSH-normal Blood urea level -75mg/dL (15-36g/dL),Serum Creatinine-3.1mg/dL (0.6-1.2mg/dL), Serum Calcium-14.0mg/dL (8.4-10.2mg/dL),Serum Albumin-3.2 g/dL (3.2-4.4g/dL),Corrected Calcium level-14.64mg/dL (8.5-10.2mg/dL),CRP-23.4mg/L (<10mg/L),Serum phosphate-2.5mg/dL (2.5-4.5mg/dL),Serum ACE Levels-Normal,Parathyroid hormone (PTH)-1.60pg/mL (15-68.3pg/mL) Vitamin D-45ng/mL (20-50ng/mL)
Chest X-ray shows mild blunting of costophrenic angle( ) 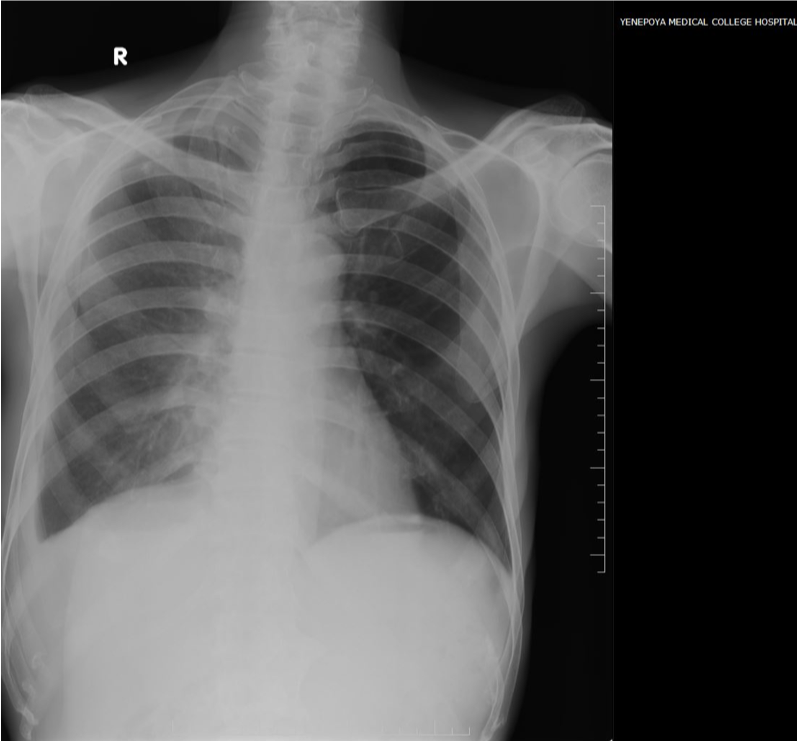
USG Neck-Thyroid gland appears normal in size and texture. No evidence of enlarged Parathyroid glands. No other significant abnormality detected CECT Thorax and abdomen-Image shows pleural thickening with enhancement
(costal, mediastinal and diaphragmatic pleura). 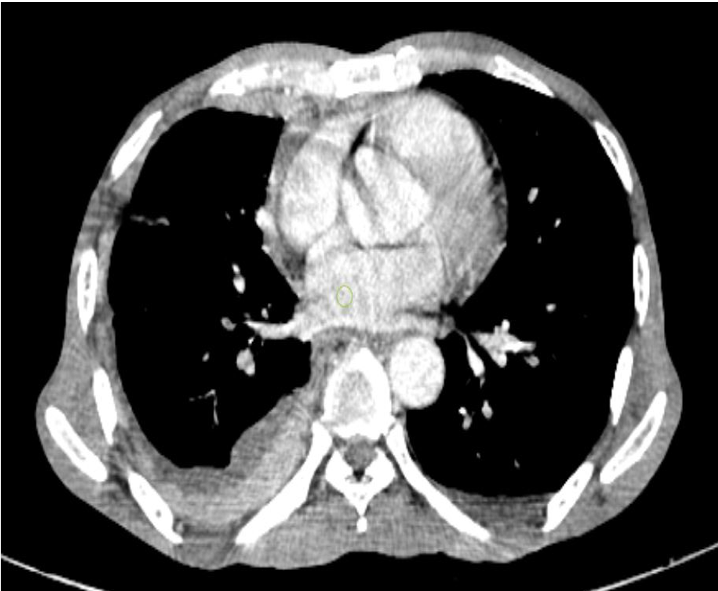
Above findings give a differential diagnosis of Koch’s Disease or Mesothelioma to be considered and suggested pleural biopsy(image enclosed) Histopathology of pleura(CT guided pleural biopsy)- Section studied show thickened pleura with numerous granuloma composed of epithelioid cells, Langhan’s giant cells and few lymphocytes-features are suggestive of tuberculosis of pleura Final diagnosis-
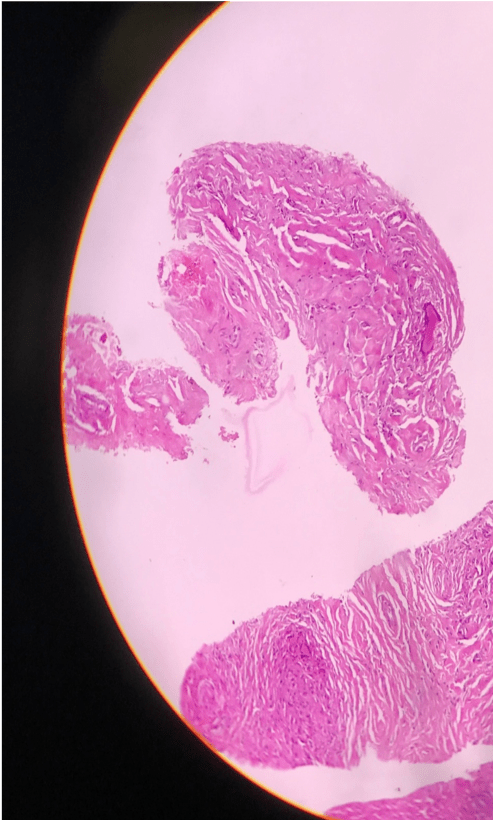
Granulomatous hypercalcemia secondary to disseminated tuberculosis
HOSPITAL COURSE
Differential diagnosis considered were: Chronic Infections-Tuberculosis/HIV, Malignancy-hematological/gastrointestinal/lung, Endocrine-diabetes,hyperthyroidism,hyperparathyroidism. On evaluation found to have severe hypercalcemia with acute kidney injury. His altered sensorium and polyuria were also explained by hypercalcemia. Such severe hypercalcemia usually occurs with malignancy. He was hyper hydrated with IV fluids. Calcitonin, furosemide, and steroids were given after correction of dehydration. Acute kidney injury resolved and calcium levels reduced. His Thyroid, PTH levels were normal. CECT thorax and abdomen was done to screen any internal malignancy /tuberculosis/sarcoidosis which showed pleural thickening which was biopsied. Biopsy revealed granuloma with caseous necrosis. ATT was started. Tapering dose of steroids were given for 4 weeks to control hypercalcemia as it was granuloma induced hypercalcemia. The patient improved symptomatically, polyuria resolved, sensorium normalized.He gained weight of 4 kg at follow up and calcium levels were 8.5mg/dl.
TEACHING MESSAGE
Though severe hypercalcemia more than 12mg/dl is commonly seen in malignancy and hyperparathyroidism reversible causes like granuloma induced hypercalcemia should be considered in a case of Pyrexia of unknown origin. Severe hypercalcemia being one of medical emergency aggressive hydration and treatment of the primary cause in our patient-led to complete reversal of his AKI, hypercalcemia, and resolution of PUO
This case was contributed by
Dr.Balachandra S Bhat,
Assistant Professor,
Dept of General Medicine,
Yenepoya Medical College
