
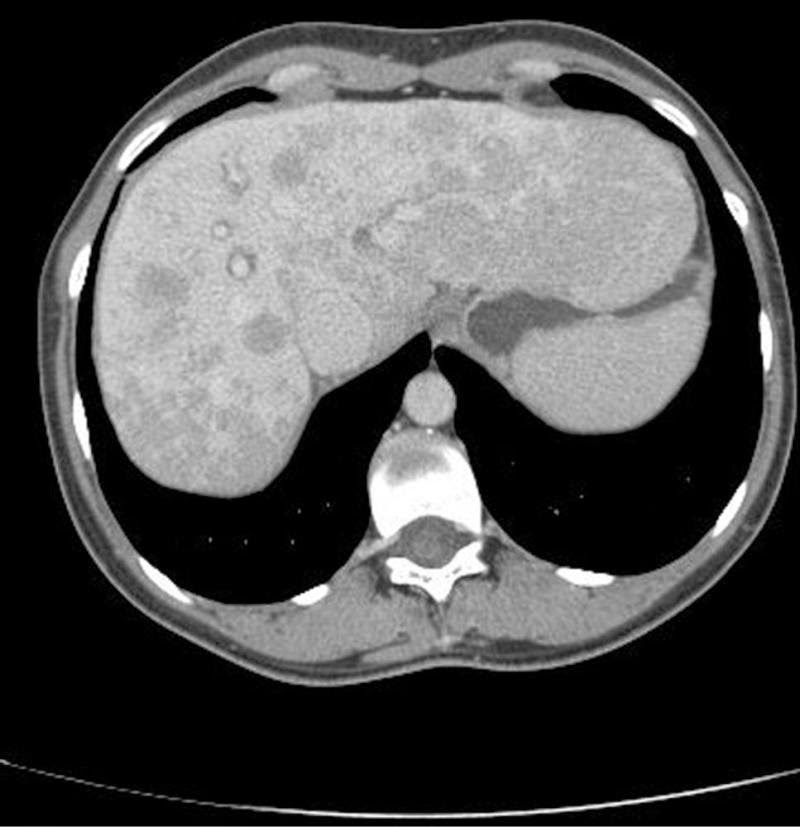
Clinical scenario: A 39-year-old female presented with a CT scan report, that read, ” multiple hypodense lesions in the liver suggestive of metastasis liver. The gall bladder, Hepatic veins, portal vein are normal. No lesion in the CBD and intrahepatic ducts are also normal”. The patient was admitted for evaluation of the primary after explaining poor prognosis to her husband thoroughly. On examination, she was conscious, oriented and deeply Jaundiced. Her vitals were stable. Her systemic examination was unremarkable.
Laboratory tests showed normal hemogram but ESR (erythrocyte sedimentation rate )was raised at 52 mm/H (normal, 0-20 mm/H). She had an elevated INR 2.7 Her liver function tests revealed predominantly conjugated hyperbilirubinemia [Bilirubin 12 mg/dl )] elevated liver enzymes (AST aspartate aminotransferase: 818U/L and ALT 51 5 U/L). Serum alkaline phosphatase levels were also elevated at 327 IU/L /L All her viral markers were negative.
All tumor markers CA -125, CEA and Alpha fetoproteins were elevated. For the search of the primary an upper GI endoscopy, colonoscopy including a mamogram was carried out. All turned out to be normal. While the search for the primary was on , day 4th of admission the patient was found to be incoherent, talking irrelevantly. Her arterial ammonia levels were high and she was shifted to ICU and managed as hepatic encephalopathy. Gladly , her sensorium improved after 3 days and a liver biopsy was planned for evaluation of liver lesions. Keeping in view her high INR 4 units of FFP were transfused and transjugular liver biopsy was done.The Liver biopsy was suggestive of Autoimmune hepatitis a great surprise to one and all.
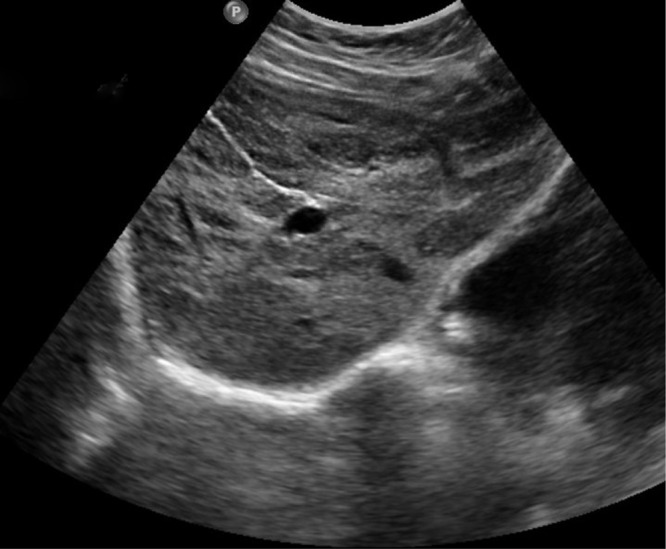
She was given oral steroids and her Liver function tests improved. Repeat Ultrasound of the abdomen showed clearance of liver lesions
One year later she was the mother of her 3rd baby.
Take-Home message
Focal liver lesions are more often discovered with the widespread use of diagnostic imaging modalities. Despite tremendous advancements in the field of radiology, radiological features are not definite. Treat the patient and not an investigation report.







